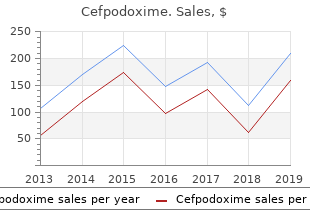
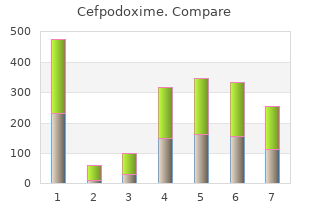
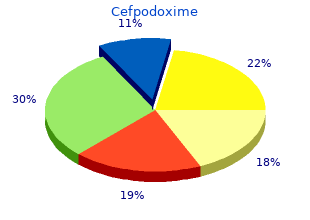
Cefpodoxime
"Buy cheap cefpodoxime 200mg on-line, antibiotic 141 klx".
By: R. Goran, M.A., Ph.D.
Vice Chair, Center for Allied Health Nursing Education
Today bacteria on tongue cheap cefpodoxime 200mg mastercard, we are able to ear infection 1 year old buy cefpodoxime on line mea sure changes occurring in the brain of those unfortunate people antibiotics before tooth extraction buy cefpodoxime without a prescription. For example, in an arm amputee, one may produce a phantom arm sensation by tickling the chin or jaw on the face on the same side as the amputa tion. These findings dem onstrate that amputation leads to a remapping of the pri mary somatosensory cortex and that one brain area can alter its functional connections, even in adults. Today, it is believed that amputation leads to three steps of change in the somatosensory cortex. This helps make the representations functional changes continue, they will eventually lead to highly specific, in saying both, �this is input from the hand� and changes in the physical connectivity between neurons. When an arm is amputated (or Normally, adjacent areas that represent different body even disabled for a long time), it leads to such a remapping of parts �. When an arm is amputated (or even tated) hand, which correlated to co-activation of both the face disabled for a prolonged time), it leads to such a remap and hand representation areas in the somatosensory cortex. When two detectors in the scanner regis ter a photon of 511keV exactly simultaneously, then a decay must have occurred on the line connecting these two detectors. At normal counting rates, the chance that two detectors simultaneously record two pho tons originating from two different positron decays is unlikely. A quantitative calcula More recently, advances have been made toward tion is possible; however, in many studies of functional functional imaging of neurotransmission; exciting activation only relative changes are recorded. The mean activity for each region 2 gained limited use, probably because an even higher for the experimental subjects would then be compared 2An electronvolt (eV) is the amount of kinetic energy gained by a single unbound electron when it passes through an electrostatic potential dif ference of 1 volt, in vacuum. Bottom panel shows 11C-raclopride binding levels (in a steady-state approach) as dopamine levels increase. The main drawback with technique used by scientists to obtain information this technique is that it takes no account of structural about the chemical and physical properties of mol brain differences which might exist between subjects. On a functional image, the inference that approaches that can measure the structure, function, structural boundaries can be identified is obviously a connectivity and chemistry of any part of the body. The human body is mostly made of processing techniques can be used to �co-register � the fat and water � body tissues that have many hydrogen imaging data on a voxel-by-voxel basis, such that a atoms. As such, the human body consists of about 65 superimposed map for each subject is obtained. Voxels are frequently used in the visualization and analysis of medical and scientific data. Zooming in on the nuclear magnetic resonance, which is a spectroscopic voxel reveals cells and within each cell there are water 2. In the brain, the resolution of the scanner determines how small the voxels can be. Parameters such as higher scanner field strengths increase the spatial resolution and hence the ability to represent separate structures in the brain. The brain voxel extracts the signal from one part of the brain, where the local molecular environment influences the magnetic response. Each water molecule consists of one oxygen imaging relies upon local dephasing of spins following atom and two hydrogen atoms. If we zoom into one of the application of a transverse energy pulse; this trans the hydrogen atoms past the electron cloud we see a verse relaxation time is termed �Time 2� or T2. In different parts of the body, such magnetic orientation of each hydrogen atom is aligned as the brain, different tissues alter the speed in which to the magnetic field and spins around this orientation T1 and T2 relaxation occurs. It is during this phase that the ning, such as the rate and amplitude of the radiofre atom loses its own energy by emitting its own energy, quency pulse, or the time from excitation to recording, providing information about the environment. The it is possible to highlight different properties of the tis relaxation occurs in two dimensions: Time-1 and Time sues and their differences. The realignment with the magnetic field is termed this can clearly be seen in images that display the dif longitudinal relaxation and the time in milliseconds ference between T1 and T2-weighted images (Figure required for a certain percentage of the tissue nuclei A. This is the basis be hard to see on a T1-weighted image is clearly vis of T1-weighted imaging, which produces the most ible on the T2-weighted image. However, the alignment is not perfect, since neighboring atoms influence each other. Brain activation Structural scanning techniques are obvious choices changes the relative concentration of oxygenated and when studying alterations in the brain due to aging, deoxygenated hemoglobin � blood with or without brain injury, or degenerative disorders such as oxygen, respectively � in the local blood supply. Furthermore, there is a non-linear relation neurons fire they consume more oxygen. When ship between age and brain volume, something that this happens, the local level of oxygenated blood contradicted the earlier views about the aging brain.
Lamotrigine as an add-on drug in the manage otrigine monotherapy for partial seizures [see comments] antibiotics for urinary tract infection during pregnancy buy 200 mg cefpodoxime. Time course of controlled infection you catch in hospital order cefpodoxime online, crossover study of lamotrigine in treatment-resistant gener lamotrigine de-induction: impact of step-wise withdrawal of carba alised epilepsy [see comments] antimicrobial wipes cefpodoxime 200 mg without a prescription. Ethosuximide, valproic acid and without valproic acid comedication: Results of a retrospective study. Does lamotrigine influence unclassifiable epilepsy: an unblinded randomized controlled trial. Lamotrigine-induced rash in chil mazepine epoxide/carbamazepine serum concentration ratios in adult dren. Single dose pharmacokinetics of carba risk/benefit considerations in adults and children [see comments]. Thepharmacokineticandpharmacodynamiccon severe cutaneous adverse reactions in lamotrigine-treated patients. The neurobiology of antiepileptic drugs for lamotrigine metabolism: evidence from double-blind placebo controlled the treatment of nonepileptic conditions. Psychiatric adverse events during therapeutics and technology assessment subcommittee and quality stan levetiracetam therapy. Side effects were also noted early due late pH-dependent activation of voltage and receptor-gated to not yet knowing the most effective dosages without side ion channels (18); its inhibitory effect is less than aceta effects. Topiramate (2,3:4,5-Di-O-isopropylidene -D neuronal injury and seizures induced by a second insult fructopyranose sulfamate). Steady-state concentrations for the same mg/kg dose were correspondingly lower in children than Renal elimination, low protein binding, and a long half-life in adults. In young children (younger than 4 years old), clearance rates were the same or slightly higher than in older children (31). Coadministration with food slightly (creatinine clearance, 30 mL/min) renal impairment com delays absorption but does not decrease bioavailability (28). Binding to plasma proteins is mini been reported when comparing age and sex-matched healthy mal (13% to 17%) and is not considered to be a major factor controls to individuals with moderate to severe hepatic in dosing and drug interactions (29). It is most important for compliance and also curonidation; none of the metabolites constitutes 5% of an if utilizing higher dose therapy. Steady-state plasma concentra administered dose, and they are quickly cleared (29). Therapeutic ranges are often quoted in the 2 to study was performed in 13 patients with epilepsy. Initial studies showed the mean serum estradiol to be reduced by 18% at 200 mg/day but repeat testing at the same 200 mg Topiramate and Carbamazepine dosage showed only an 11% decrease. The mined in 12 adults whose epilepsy was stabilized with carba level of induction is substantially less than that associated mazepine 300 to 800 mg t. No significant differences with potent enzyme-inducing agents such as carbamazepine were observed in the pharmacokinetics of total or unbound (42% reduction in estrogen concentration) (41). Changes in metformin pharmacokinetics 2 years, 30% at 3 years, and 28% at 5 years (64,65). Adjunctive Therapy With a mean daily dose of 6 mg/kg (target dose, 5 to 9 mg/ kg/day), median seizure reduction was 33% (placebo, 11%; Partial-Onset Seizures P 0. All 83 children completing the double-blind phase entered Similarity of trial design and patient populations allowed the long-term, open-label extension in which the dosages of pooled analysis of data from six of these trials (51�56). During open-label in-prac seizure free, while no patients in the placebo group were tice studies in children with refractory partial-onset seizures seizure free (P 0. On initial review of the data, it appeared that there was a flat Lennox�Gastaut Syndrome tening of the efficacy curve at higher dosages. Therefore, from an efficacy point of view, there was a median reduction for drop attacks was 15% compared with a dose�response curve. During the last 6 these outcomes compared favorably with those reported for months of treatment, 16% had no generalized tonic�clonic lamotrigine in this population (73). In addition, the frequency of tonic�clonic seizures plus at least one other type of generalized myoclonic seizures was reduced and the number of weeks seizure.
Any differences in the colour of the two irides (heterochromia iridis) should be noted as this may indicate congenital Horner�s syndrome infection 2004 buy discount cefpodoxime 100mg on line, certain ocular inflammatory conditions (Fuch�s heterochromic cyclitis) antibiotics for uti treatment order cefpodoxime overnight delivery, or an intraocular Distorted pupil after broad foreign body antibiotic resistance nature journal order cefpodoxime 100mg line. The position of the corneal reflections helps to confirm whether there is a true �squint. If so, they should be asked to say whether diplopia occurs in any particular direction of gaze. It is important to exclude palsies of the third (eye turned out) or sixth (failure of abduction) cranial nerves, as these may be secondary to life threatening conditions. Complex abnormalities of eye movements should Eye movements lead you to suspect myasthenia gravis or dysthyroid eye disease. The presence of nystagmus should be noted, as it may indicate Test movements in all directions significant neurological disease. Convergence Test eye movements in all directions and when converging the cornea should be stained with fluorescein eye drops. Normal position of corneal light reflexes If this is not done, many lesions, including large corneal ulcers, may be missed Eyelids, conjunctiva, sclera, and cornea Examination of the eyelids, conjunctiva, sclera, and cornea should be performed in good light and with magnification. You will need: a bright torch (with a blue filter for use with fluorescein) or an ophthalmoscope with a blue filter a magnifying aid. The lower lid should be gently pulled down to show the conjunctival lining and any secretions in the lower fornix. Corneal abrasion stained with the anterior chamber should be examined, looking fluorescein and illuminated with specifically at the depth (a shallow anterior chamber is seen in blue light angle-closure glaucoma and perforating eye injuries) and for the presence of pus (hypopyon) or blood (hyphaema). All these signs indicate serious disease that needs immediate ophthalmic referral. Eyelids�Compare both sides and note position, lid If there are symptoms of �grittiness,� a red eye or any lesions, and conditions of margins history of foreign body, the upper eyelid should be everted. Ectropion Basal cell carcinoma Blepharitis 4 History and examination this should not be done, however, if there is any question of ocular perforation, as the ocular contents may prolapse. Conjunctiva and sclera�Look for local or generalised inflammation and pull down the lower lid and evert upper lid. The drainage angle of the eye can be checked with a special Scleritis: localised redness lens (gonioscope). Conjunctivitis: generalised Blood in anterior chamber redness (hyphaema) Intraocular pressure Assessment of intraocular pressure by palpation is useful only when the intraocular pressure is considerably raised, as in acute closed angle glaucoma. The eye should be gently palpated between two fingers and compared with the other eye or with the examiner�s eye. Special contact lens being used to view the drainage angle of the eye (gonioscope) Ophthalmoscopy Good ophthalmoscopy is essential to avoid missing many serious ocular and general diseases. Specific contact and non-contact lenses are used during the examination, and the ophthalmologist should use a slit-lamp microscope or head-mounted ophthalmoscope. There is an associated risk of precipitating acute angle closure glaucoma, but this is very small. The best dilating drop is tropicamide 1%, which is short acting and has little effect on accommodation. However, the effects may still last several hours, so the patient should be warned about this and told not to drive until any blurring of vision has subsided. The patient should be asked to fix their gaze on an object in Measuring intraocular pressure by applanation tonometry the distance, as this reduces pupillary constriction and accommodation, and helps keep the eye still. To enable a patient to fix on a distant object with the other eye, the examiner should use his right eye to examine the patient�s right eye, and vice versa. This red reflex is the reflection from the fundus and is best assessed from a distance of about 50cm. If the red reflex is either absent or diminished, this indicates an opacity between the cornea and retina. The optic disc should then be located and brought into Patients should always be warned to seek help immediately focus with the lenses in the ophthalmoscope. If a patient has a if they have symptoms of pain or haloes around lights, high refractive error, they can be asked to leave their glasses on, after having their pupils dilated although this can cause more reflections.
It is best to going off antibiotics for acne cheap 100 mg cefpodoxime amex start with a somewhat distal target in order to antimicrobial zone of inhibition generic 100mg cefpodoxime otc preserve vein length for subsequent anastomoses 6 bacteria kid definition discount cefpodoxime 200mg fast delivery. Assessment Tools for Session 4 the entire procedure including briefing and de-briefing should be videotaped and submitted. Prerequisites Each resident will have successfully completed the homework assigned in Session 4. The resident will note target temperature and institute antegrade cardioplegia (retrograde will not be used due to time constraints). Measure the appropriate length of vein for each graft and anastomose to the aorta. After the last bypass has been completed (distal and proximal), discontinue cardioplegia, de-air the grafts, wean from cardiopulmonary bypass, and de-cannulate. The technical aspects of aortic valve replacement are broken down into their component parts which are learned and practiced at each weekly session and between sessions. The goal of this module is not only to have performed aortic valve replacement but also to have practiced the component steps enough to demonstrate basic proficiency in them. The resident will be able to describe the anatomy of the aortic root and the important relationships that exist. The resident will be able to perform and close an aortotomy (transverse/hockey stick) 3. The resident will be able to excise the aortic valve, size the annulus, place annular and valvular sutures, seat and tie down the sutures and assess appropriate positioning (with a score of 5 for all steps). The schedule of the components of training is as follows: Session 1: Anatomy, Aortotomy and Closure of the Aorta Videos/presentations � Grossi/Northrup/Hicks (see p. Session 3: Deairing of the heart Introduction of standardized method of de-airing the heart after cardiotomy. Multiple repetitions of deairing procedure using the Ramphal Cardiac Surgery Simulator. Decannulation at end of last procedure Residents should have ample opportunity to practice between weekly sessions. Each session will begin with an evaluation of the component tasks covered in previous sessions. This session will teach the fundamentals of the aortotomy and closure of the aorta. The resident will be able to dissect the heart in such a way as to point out the anatomic features critical to safe aortic valve replacement. The Grossi and Northrup presentations should be played and visible to the resident. There should be capacity to readily start and stop the videos so that resident will have the time to study the anatomy. Any deficiencies in the videos or the dissection models Residents will receive guidance and formative feedback from the faculty during the exercises. Residents will provide feedback regarding perceived relevance of assignments and validity of tasks. In addition, the resident will learn to place stitches through the valve and properly orient and seat the valve. The resident will learn to tie the stitches on both mechanical and bioprosthetic valves Prerequisites Session 1 objectives performed satisfactorily. Place 4th set of sutures through the sewing ring of a mechanical valve with proper spacing and tie it down. Place 5th set of sutures through the sewing ring of a bioprosthetic valve with proper spacing and tie it down. This session will utilize the pressurized pig heart to teach the resident the steps of air evacuation after cardiotomy. The resident will be able to initiate cardiopulmonary bypass and cardiac arrest (without air in the circuit or heart) 2. The resident will be able to adequately remove air from the heart after aortotomy Prerequisites Read Chapter 12, Extracoporeal Circulation, by Drs.
During the rhythmic activity antibiotic resistance research topics cefpodoxime 200mg low price, the patient responded appropriately to virus x movie cheap cefpodoxime 200 mg otc an auditory stimulus (clicker) treatment for sinus infection in toddlers cheap cefpodoxime 100 mg overnight delivery. In the last channel, the upward deflection was from the technician�s sound stimulus, and the subsequent downward deflec tion was from the button pressed by the patient in response. The patient remained awake and responsive throughout the recording and afterward recalled the test word (�auto�). Note the general ized, rhythmic, high-amplitude theta activity with intermixed sharp transients during drowsiness. She was misdiagnosed as having absence epilepsy because of hyperventilation induced high-amplitude rhythmic slowing. The girl was alert and responsive during this tracing, which was obtained after 2 minutes of hyperventilation. Note the asymmetry of background rhythms owing to the since 4 years of age, seizure free on medication for the last 1. Note the time-locked, unsustained, bioccipital response to 8 and 4-Hz photic stimulation, separated by normal posterior background activity. Photic driving represents a normal response to photic stimu lation and is not related to the epilepsy of the patient. These generalized 3-Hz spike-and-wave complexes were precipitated by hyperventilation and lasted for 4 seconds, with staring and unresponsiveness. She was seizure free throughout adulthood until absence status epilepticus began during chemotherapy for breast cancer. During this episode, with generalized polyspike-and-wave complexes, she had unresponsiveness and eyelid fluttering. Electroencephalographic findings and behavior returned to normal after intravenous injection of diazepam. She had no previous history of seizures, and this was her first manifes tation of generalized absence epilepsy. This episode began with repeated myoclonic jerks of the 2 weeks before this electroencephalogram. Note the polyspike compo arms and upper body synchronous with the generalized spike-and nent of the spike-and-wave complexes during the myoclonic jerk wave complexes. This flurry evolved after 20 seconds into a general precipitated by photic stimulation. Note the generalized high-amplitude slow transient followed by a generalized electrodecremental pattern for 3 seconds. The spasm involved tonic abduction and extension of both arms with flexion of the trunk and neck. Note the bifrontal polyspikes preceding the retardation and intractable generalized tonic, atonic, myoclonic, and generalized sharp and slow-wave complexes (5), also called slow atypical absence seizures since age 4 years. Interictal electroencephalogram showed generalized sharp and slow wave complexes. Two seizures are recorded here, with limp head nod ding plus tonic stiffening and elevation of both arms. Each seizure began with a generalized sharp wave (arrows) fol lowed by attenuation of electroen cephalograph activity and cessation of muscle artifact. During this electroencephalography, the patient was mon in children with clinical features similar to those of reading; note the horizontal eye movement artifact. Note that the sharp waves were showed normal findings, but recording during drowsiness and light reflected at the scalp as dipoles, with maximum negativity over the left sleep showed left centrotemporal sharp waves (benign focal epilepti centrotemporal region and maximum positivity over the vertex. Many children with benign focal Dipole potentials are typical of benign focal epileptiform discharges of epileptiform discharges of childhood do not have seizures (19), and childhood, possibly as a result of horizontal orientation along banks the finding may be incidental. Benign focal epileptiform discharges of childhood are commonly bifocal or multifocal, often from homologous areas of both hemispheres (18). The right occipital sharp waves with typical mor phology of benign focal epileptiform discharges of childhood (18) were abundant in light sleep but rare during wakefulness. Interictal electroencephalogram showed sharp waves from the right anterior temporal region, with maxi mum amplitude at electrode F8. Episodes involved a subtle change of facial expression and decreased responsiveness with minimal or no automatisms (�hypomotor� symptoma tology, as discussed in Chapter 14).
Purchase generic cefpodoxime line. Microbiology Antimicrobials.